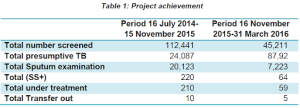
The TB REACH project aims to increase case finding among high risks groups (garbage collectors, street children, TB suspects who visited private pharmacies, and contacts of TB patients) in Kathmandu Valley. A total number of 157,652 (Male = 76,706, Female = 80,946) people were screened from project sites from 16 July 2014-15 March 2015-2016. Among the total screened using a standard questionnaire 21% (32,879) were found to be presumptive TB. Among presumptive TB identified from the door-to-door visit, approximately eighty-three percent (27,346/32,879) participated with sputum samples in the microscopy camps or nearby laboratories. The remaining 17% could not participate in the microscopic camps or laboratories due to the following reasons; a busy working hours from early morning to the late evening, difficulty to discharge quality sputum samples, the existence of social stigma in the local community, and submission of a poor quality sputum samples. Due to the improved access to the diagnosis, 86% of female presumptive TB cases participated in the sputum microscopic camp compared to 80% of males.
In total 284 cases (PPM 193, Garbage collectors 49, street children 6, contacts of TB patients 24 and self-visited or other than above mention groups 12) were diagnosed as sputum smear-positive (SS+) TB of whom 269 enrolled their treatment in project intervention districts and 15 cases transferred out to other districts where they need to travel back to their home due to the family reasons and poor health status. Among the total examination, the positivity rate of sputum smear-positive (SS+) TB was 1.03%.
The active involvement of Female Community Health Volunteers (FCHV), Health Care providers (public and private), and other stakeholders is essential to achieve above-mentioned progress in Kathmandu Valley.
Joint planning of project activities with key stakeholders and sharing of progress with NTP on regular basis is another beauty of this project. The project always welcomes and highly acknowledges logical feedback for the betterment and effectiveness of the intervention. The intensive involvement of health volunteers and workers in the community provides support to establish social harmonization with community people. The regular door-to-door visit activity by volunteers supports minimizing the stigma and discrimination related to TB. People living with TB symptoms to consult with project staff including local volunteers and health workers without any hesitation.
The project learned intensive community mobilization approach is very much helpful in big cities like Kathmandu where diverse healthcare facilities are providing TB diagnosis and treatment services on their own without following NTP policy and guidelines.